 |
New: MEN'S HEALTH & LONGEVITY 101
"The Cousin Sal Minute... or Two"- on Prostate Screening
6/11/2024- I recently partnered with "PROSTATESCAN NOW" because of the rampant health concern in my generation and my retired FF community for Proscate Cancer. I welcome you to view our pilot episode in support of proactive checkups and Prostate Health! I'm speaking to all my dude-friends in their 50's who need to start taking their health more seriously, while applauding those who have stayed on top of early detection and prevention. One such person is my latest hero in this- Mr. Barrie Kolstein. Check out our feature on this great motivator and role model! (See video)
For slow-growing cancers such as prostate, breast, kidney, and thyroid cancer, monitoring cancers during its very early stages (instead of immediate treatment) may be a good option. This means closely watching a patient’s condition but not giving any treatment unless there are changes in test results that show the condition is getting worse. Active surveillance may be used to avoid or delay the need for treatments such as radiation therapy or surgery, which can cause side effects or other problems. During active surveillance, certain exams and tests, such as blood tests, imaging tests, and biopsies, are done on a regular schedule to monitor the condition. Active surveillance may be used in certain types of prostate cancer and in some other types of cancer. It is a type of expectant management. (See complete info)
| Special Articles & Reports (2024) | |
 |
THE WILD WEST OF PSA TESTING:
HOW EFFECTIVE ARE STRATEGIES TO LOWER PSA READINGS? By: Dr. Roberta Kline PSA, or prostate-specific antigen, is a protein produced by prostate cells. It can be elevated when these cells increase in number and is a common screening test for prostate cancer. Studies have shown that up to 75% of men with elevated PSA levels do not have prostate cancer on biopsy, however, and up to 50% of prostate cancers are overdiagnosed... (see complete report) |
 |
PILOT STUDY ON THE ROAD (part 1) Sal Banchitta, one of four volunteers took home the Nova-HD (by AuraWell PEMF) from the Bard Diagnostic Imaging center in NYC. All case studies are instructed to use the PEMF device as directed- applying electromagnetic exposure via the provided PEMF coil for an est. 20 minutes 2x a day. "Aside from the clicking sound of the power source device, what I learned about PEMF is that it's widely known to be painless and has no known side effects", says Mr. Banchitta. "I also learned this technology to offer so much by ways of pain relief and cell regenerative therapy". |
 |
IMAGE GUIDED APPROACH TO THE TREATMENT OF PROSTATE HYPERPLASIA(4-Case Performance Study) by: Robert L. Bard, MD Procedurally, the best way to study an enlarged hyperplastic prostate gland is as a low grade inflammatory process, similar to women with fibrocystic breasts considered to be breast inflammation. [1] This does not need to be treated with antibiotics since this inflammation is often aligned with a chronic disease and requires a long-term treatment protocol. One example of this therapy is using a pulse electromagnetic applicator (PEMF) which can be applied over the groin area or under the pelvis (even in the car seat). For treatment applications, this protocol is recognized to be safe, painless, comfortable, and user-friendly on a long-term basis. (see full report) |
How Reliable is PSA TESTING? (source: NIH/NCBI)
PSA (prostate-specific antigen) testing (for elevated levels) is designed to detect prostate cancer at its early stages. But to clarify, reports indicate that a wide range of men with high PSA levels does not preclude cancer. At best, shows a possible alert to get an ultrasound scan (or a prostate biopsy).
Prostate cancer, now considered the most common cancer in men, especially African-Americans (6-NIH), was rare until the 1950’s. Earlier, a blood test identifying prostate specific antigen (PSA was developed for use in “rape kits” to provide criminal evidence in court) was never designed as the screening tool for prostate cancer that it has become today. Our national guidelines recommend screening with PSA for men age 55 to 69, a recommendation that 40% of men follow. But what happens after a PSA test is termed positive?
CALLING FOR A DIAGNOSTIC UPGRADE
The strategy of relying on a (PSA) blood test as the precursor to a biopsy required significant reassessment. Though approved by the FDA in 1986 as the gold standard for monitoring cancer relapses, increasing reports continue to indicate that elevated PSA levels in over 70% of men show a false positive reading- and does not conclude a malignant cancer. (NIH ref). Because of the inaccuracies of the PSA test and the risk of side effects, many centers are now using imaging solutions like ultrasound 3-D Doppler and MRI before considering a biopsy. (see complete article)
 |
According to the American Cancer Society, prostate cancer is the second most common cancer in American men. Estimates for prostate cancer in the United States for 2019 are estimated at about 174,650 new cases of prostate cancer and about 31,620 deaths are expected from prostate cancer. About 1 man in 9 will be diagnosed with prostate cancer during his lifetime. The average age at the time of diagnosis is about 66.Prostate cancer is the second leading cause of cancer death in American men, behind lung cancer. About 1 man in 41 will die of prostate cancer. Prostate cancer can be a serious disease, but most men diagnosed with prostate cancer do not die from it. In fact, more than 2.9 million men in the United States who have been diagnosed with prostate cancer at some point are still alive today.
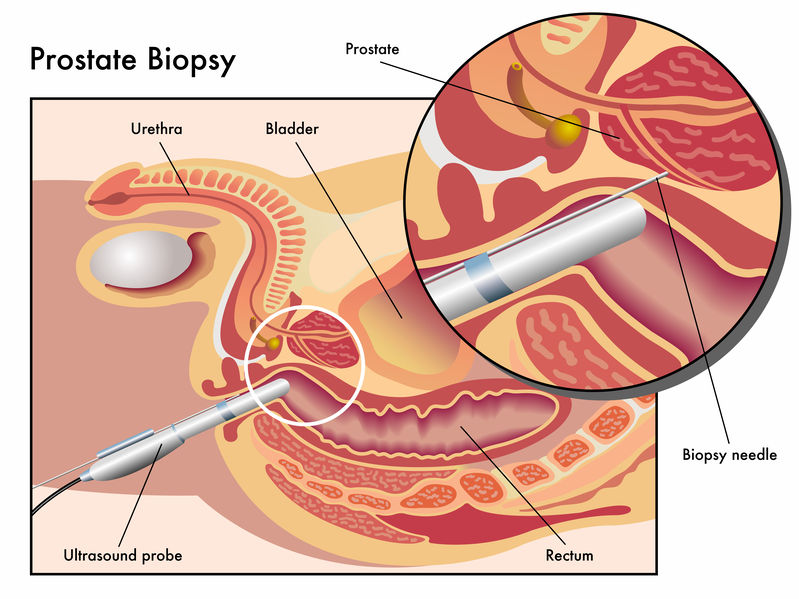
Most prostate cancers found by screening are small and slow growing and may not be fatal. Some men may have a faster growing prostate cancer and will benefit from early treatment. Older men, African-American men, and men who have a family history of prostate cancer have a greater risk for developing prostate cancer. If you are concerned that you may have a greater risk for prostate cancer, talk to your doctor about screening. One screening test for prostate cancer is a blood test, which can be abnormal (not normal) for several reasons besides prostate cancer. The only way to know if an abnormal test is due to cancer is to do a biopsy. A biopsy is a surgery to get small pieces of the prostate to look at under a microscope. If the biopsy shows there are cancer cells, then your doctor will discuss treatment options. (Source: CDC.gov)
WHAT IS SCREENING?
 |
See complete article at the NIH (National Cancer Institute) Website
Screening is looking for cancer before a person has any symptoms. This can help find cancer at an early stage. When abnormal tissue or cancer is found early, it may be easier to treat. By the time symptoms appear, cancer may have begun to spread. Scientists are trying to better understand which people are more likely to get certain types of cancer. They also study the things we do and the things around us to see if they cause cancer. This information helps doctors recommend who should be screened for cancer, which screening tests should be used, and how often the tests should be done.
It is important to remember that your doctor does not necessarily think you have cancer if he or she suggests a screening test. Screening tests are given when you have no cancer symptoms. Screening tests may be repeated on a regular basis. If a screening test result is abnormal, you may need to have more tests done to find out if you have cancer. These are called diagnostic tests.
Different factors increase or decrease the risk of developing prostate cancer.
Anything that increases a person's chance of developing a disease is called a risk factor. Anything that decreases your chance of getting a disease is called a protective factor.For information about risk factors and protective factors for prostate cancer, see the PDQ summary on Prostate Cancer Prevention.
KEY POINTS of Prostate Cancer Screening
• Tests are used to screen for different types of cancer when a person does not have symptoms.
• There is no standard or routine screening test for prostate cancer : Digital rectal exam or
Prostate-specific antigen test
• A prostate cancer gene 3 (PCA3) RNA test may be used for certain patients.
• Screening tests for prostate cancer are being studied in clinical trials.
 |
Tests are used to screen for different types of cancer when a person does not have symptoms.
Scientists study screening tests to find those with the fewest harms and most benefits. Cancer screening trials also are meant to show whether early detection (finding cancer before it causes symptoms) helps a person live longer or decreases a person's chance of dying from the disease. For some types of cancer, the chance of recovery is better if the disease is found and treated at an early stage.
There is no standard or routine screening test for prostate cancer.
Although there are no standard or routine screening tests for prostate cancer, the following tests are being used or studied to screen for it:
Digital rectal exam
Digital rectal exam (DRE) is an exam of the rectum. The doctor or nurse inserts a lubricated, gloved finger into the lower part of the rectum to feel the prostate for lumps or anything else that seems unusual.
See complete article at the NIH (National Cancer Institute) Website
| © Cancer Research UK [2002] All right reserved. Information taken 03/09/19 | What are the Signs and Symptoms of Prostate Cancer? | Cancer Research UK Find out the signs and symptoms of prostate cancer from Cancer Research UK. Learn how prostate cancer is diagnosed and the tests needed to find out. https://www.cancerresearchuk.org/about-cancer/prostate-cancer/symptoms. In the video, Dr. Vincent Gnanapragasm from Cambridge University talks us through prostate cancer symptoms, signs and types (more)
|
TODAY'S RADIOTHERAPY: CYBERKNIFE TECHNOLOGY (part 1)
 Demo video courtesy of www.CancerScan.com |
MEETING TODAY’S CHALLENGES FOR CANCER THERAPY
Since the advent of radiation therapy (and the invention of the x-ray) over a century ago, the noninvasive treatment approach of radiotherapy continues to be recognized as one of the most forward-thinking technologies in the pursuit of targeting cancer tumors. The CyberKnife® Robotic RadioSurgery System represents the latest performance innovation in this modality for treating benign and malignant tumors as well as other chronic disorders. To review the CyberKnife technology, we approached the Perlmutter Cancer Center at NYU Winthrop Hospital—the top radiotherapy and CyberKnife cancer treatment center in the country. Michael C. Repka, MD, a radiation oncologist there, shared his extensive insight and firsthand experience about CyberKnife technology including its performance and patient benefits.
THE INTEGRATIVE REVOLUTION
The CyberKnife® system combines three different technological advances. The first is x-ray based or photon based radiation, the standard form—and vast majority—of medically induced radiation. This is delivered by a linear accelerator, a device that generates high energy x-rays that are far higher in intensity than a CT scan or a conventional x-ray. The CyberKnife combines a miniaturized linear accelerator (rather than the typical oversized linear device), to allow room for a second technological advance—the integration of a robotic arm, known as a manipulator. The third advance is equipping CyberKnife with an interactive image-guidance system that acquires stereoscopic kV images during treatment. (see complete article)
Source: NYCRA News
INNOVATION REPORT: The Power Doppler Sonography
| Demo video courtesy of www.CancerScan.com |
When imaging detects a region of interest or suspicion, it can also be used to direct selective biopsies to obtain very small tissue samples for further laboratory analysis (pathology). The use of imaging together with pathology gives the most accurate information about the size, location and aggressiveness of any cancer thus identified.
Until recently, standard prostate cancer screening consisted of a PSA blood test (Prostate Specific Antigen) and DRE (Digital Rectal Exam). In 2017 a U.S. Government Panel released a statement suggesting such screening had a high cost with doubtful survival advantage. In other words, too many men whose screening revealed a suspiciously high PSA or abnormal DRE were rushed into multi-needle biopsies that entailed risks of false negatives, infection, and sexual side effects. The Panel recommended discontinuing routine PSA screening unless men had known risk factors for prostate cancer; and the American Urological Association recommended that doctors discuss the costs of PSA screening with their patients before administering the blood test.
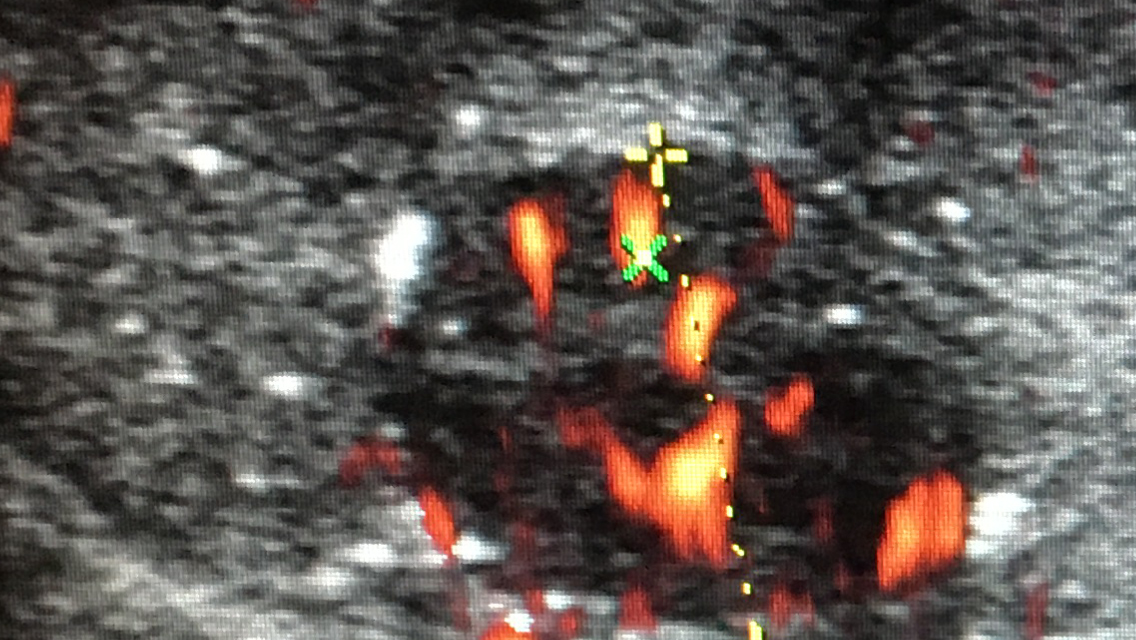
Introducing the Power Doppler Sonography of the prostate, a non-invasive way to screen for prostate tumors with their abnormal blood vessels. It actually shows any suspicious area so it can be selectively targeted for biopsy. This eliminates the so-called blind biopsy (Transrectal Ultrasound or TRUS-Guided biopsy) which often misses cancer because ordinary ultrasound can’t distinguish tissue with accuracy. The precision of a targeted biopsy eliminates the need for a large number of random needles. Histogram volumetric tumor vessel analysis on a dedicated workstation correlates with microscopy and is used as a substitute tumor marker to quantify tumor virulence noninvasively. 3D Doppler imaging offers the following advantages:
• Accuracy 95% (greater than MRI at 80-90%)
• 1000-1500 images obtained in 5-10 minutes painlessly
• 2 x more accurate for detecting spread of tumor outside gland than MRI
• Optional 3D Histogram Analysis of Vessel Density indicative of tumor aggression
• Non-invasive non-biopsy modality to verify tumor treatment response
• Submitted MRI, bone and CT scans reviewed as part of the consultation
Source: CancerScan.com
 |
Hey Fellas... WHAT TIME IS IT?
If you are with that age range of 45-50, it may be time to start a regimen of Prostate Cancer Screening as part of EARLY DETECTION. Staying regular witrh checkups greatly decreases the risk of getting malignant cancers, while improving the chances of success for those under treatment. In the ongoing battle against cancer, it is common knowledge that most cancers in their early stages are far more likely to be treated with positive results. Moreover, a thorough checkup of one's physiological analyses, heredity review and personal data gathering (from blood & dna tests) are all strong info-gatherings for early warning signs that someone may be a candidate for cancer. Being PROACTIVE starts with AWARENESS, EDUCATION & SCREENINGS.
![]()
 Mr. James Hunt- researcher and educational advocate for Prostate Cancer Survivorship www.AwarenessforaCure.org Mr. James Hunt- researcher and educational advocate for Prostate Cancer Survivorship www.AwarenessforaCure.org |
WINNING MY BATTLE WITH PROSTATE CANCER
STARTS WITH A SECOND OPINION
PROACTIVE CANCER RESEARCH & THE DIGITAL BIOPSY by: James Hunt (see full interview at: Survivor Stories / Awareness for a Cure)- originally published - March 14, 2018)
I want to tell my story so that I can help others diagnosed with prostate cancer. This all started with a routine physical with blood work. My primary care physician called to say everything looks good except a slightly elevated PSA and suggested I make an appointment to see a urologist. After spending months on antibiotics to treat a possible infection of the prostate due to bike riding, my urologist suggested a biopsy. The biopsy was one of the worst things I’ve ever experienced in my life. The biopsy results showed a Gleason 6 cancer in one of the 12 tissue samples taken from me.
The urologist suggested active surveillance where we would monitor the cancer with blood tests, MRI’s and biopsies. He mentioned that I would eventually need surgery- probably within a year or two. I reached out to one of my chiropractor friends for some advice (Dr. Mark Jones of Wading River) who is quite knowledgeable in Holistic medicine and he suggested; Pomi-T a dietary supplement that was used in a study (in prison) that was proven to slow the growth of prostate cancer. He also told me about Chaga Tea - brewed from the Chaga mushroom that grows on birch trees in Canada. I connected with Debbie Falborn from Chaga Island who told me "we will beat this". They helped me put together a plan that consisted of drinking 24oz of chaga tea a day along with daily supplements of Glutathione, Vitamin B complex and Magnesium powder (Calm). See 2021 Video Interview.
(see full interview at: Survivor Stories / Awareness for a Cure)
|
 |
ABOUT NYCRA
The New York Cancer Resource Alliance (NYCRA) is a self-funded union of volunteers comprised of caregivers, accredited medical professionals, cancer educators, publishers and published experts, patient support clinicians and non-profit foundation partners whose united mission is to bring public education and supportive resource information to the community of patients, survivors and any individual(s) seeking answers about cancer. NYCRA is an exclusive, non-commercial private network originally established on the LINKEDIN digital society and is supported by the alliance whose mission is to share informative materials to the community. For more information, visit: www.NYCRAlliance.org
Disclaimer & Copyright Notice: The materials provided on this website are copyrighted and are the intellectual property solely of the publishers/producers ( the NY Cancer Resource Alliance and IntermediaWorx inc). The contents in this website are completely INFORMATIONAL and are provided solely for your own personal, non-commercial use and not for purposes of resale, distribution, public display or performance, or any other uses by you in any form or manner whatsoever. The publishers/producers of this website and the contents of this website such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 911 immediately.
Unless otherwise indicated on this Internet web site, you may display, download, archive, and print a single copy of any information on this Internet web site, or otherwise distributed from us for such personal, non-commercial use. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages, in the Terms of Use or in the Additional Information section of our Site (which his incorporated herein by reference). This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.