
 Excerpted from "PinkSmart news" Excerpted from "PinkSmart news" |
|||
|
TAMOXIFEN vs. AROMATASE INHIBITORS FOR MALE BREAST CANCER In a private conference hosted by the Male Breast Cancer Global Alliance, our NYCRANEWS editorial team met Dr. Jose Pablo Leone, medical oncologist and researcher at the Dana-Farber Cancer Institute. Discussions covered tamoxifen and aromatase inhibitors for the treatment of male breast cancer, and his research plans in this field. BACKGROUND Currently, Tamoxifen remains the only standard of care that is available for men with breast cancer. Dr. Leone started his review on Tamoxifen vs AI in 2014 in the University of Iowa at the VA hospital where he encountered with many cases of men who had breast cancer undergoing treatment. His interest widely expanded due to the lack of data on how to successfully manage and treat male breast cancer. INTERVIEW WITH Dr. LEONE:
There are so many other endocrine therapy options available that are available to women with breast cancer, but none apply for men prior to Tamoxifen. Tamoxifen is recognized as a very good drug and an effective drug for the treatment of breast cancer and both in men and in women. Current research on Tamoxifen for men is designed to collect reactive data to support the exploration of further options. Tolerance levels vary between men, some showing minimal or no side effects, but others display significant and profound adverse effects. HOT FLASHES for both genders are common with this drug. But as opposed to women who may already have undergone menopause and are familiar with this experience, men have a tough time coping with this issue. In addition, other men-specific side effects appear in higher incidents like fatigue, erectile dysfunction and also the risk of blood clots or deep venous thrombosis or thromboembolic events. These appear higher in men than in women, causing the demand for investigation. For women, other endocrine therapies exist beyond Tamoxifen. Aromatase inhibitors are a common option either prior to or instead of Tamoxifen. Postmenopausal women can use Tamoxifen for a couple of years and an Aromatase Inhibitor after within a five-year treatment schedule as part of a standard endocrine therapy. Meanwhile, others can use only AI inhibitors for the full five years. Due to the physiological differences in the endocrine system between men and women, there may be differences in the efficacy of aromatase inhibitors, leaving men with only Tamoxifen as their primary option. Tamoxifen for men is the standard recommended drug for men with metastatic breast cancer. If there is progression of disease after Tamoxifen, then other endocrine therapies can be used in the metastatic setting. This is why we need prospective studies evaluating AI in men. We are working on a clinical trial of endocrine therapy for male breast cancer. The study will be done in collaboration with the TBCRC and the Male Breast Cancer Global Alliance. This trial comes from the essential question that we face every day when we take care of men with breast cancer as far as Tamoxifen and alternatives. |
||
 |
SURGICAL EVOLUTION IN BREAST CANCER LOCALIZATION: WIRE-FREE RADAR IMPLANTS Wire-free Radar Localization is a pre-surgical procedure to locate and mark the exact breast abnormality through the use of a small, 12×1.6 mm implanted radar reflector device, roughly the size of a grain of rice. This micro-electronic implant communicates with the scanning handpiece, allowing the surgeon to identify the exact tissue (and how much of it) to extract during a lumpectomy [1]. In this feature article, we present Dr. TroyShell-Masouras of Paradise Coast Breast Specialists in Naples Fla. - and David Gilstrap, Director & Global Product Management of Merit Medical. Together, we explored technical perspectives and design strategies behind radar localization and the SCOUT® technology. They shared the procedural advantages provided by the wire-free upgrade as well as its overall improvements to the patient's well-being in the pre and post-surgical phases. (See feature article) |
||
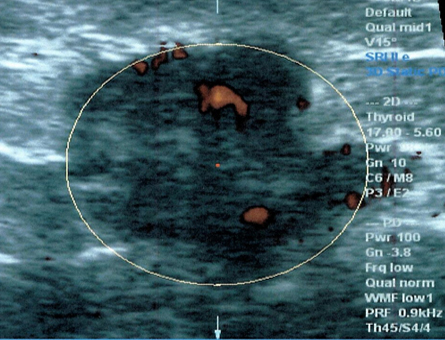
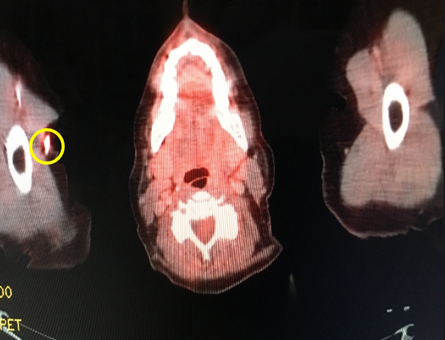
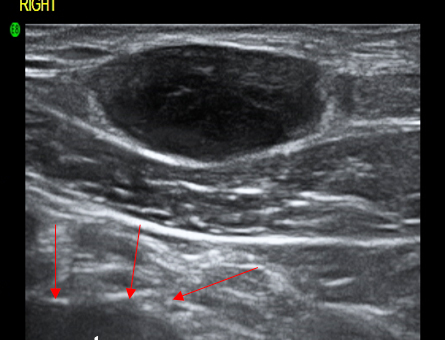
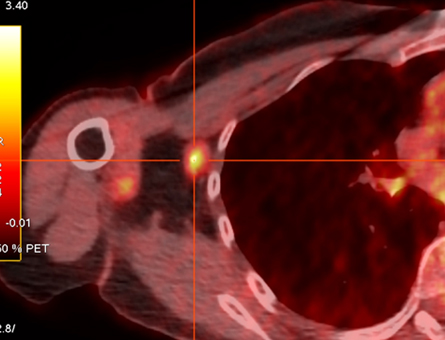
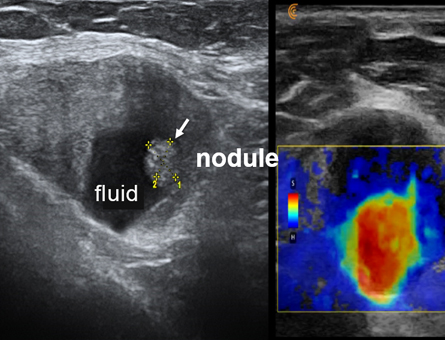
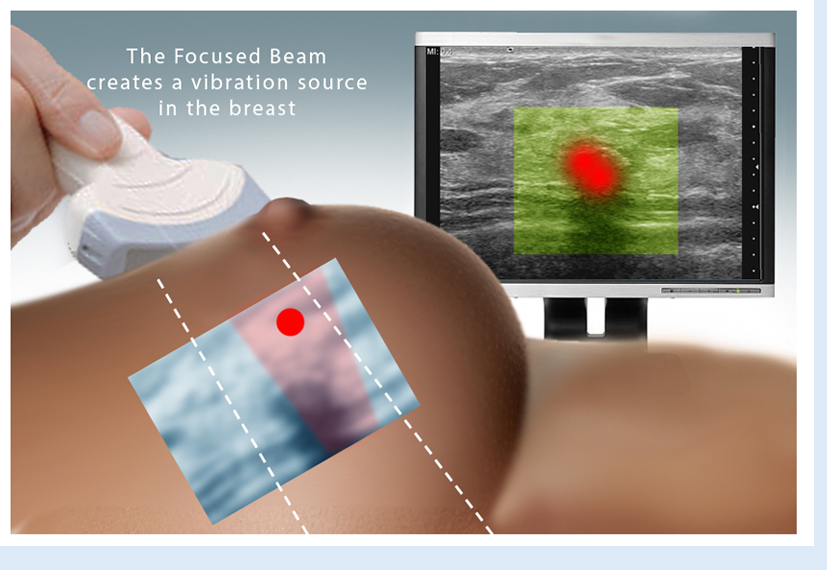
| CLINICAL IMAGING OF BREAST CANCER Explained (click thumbnails for enlarged slide show) | |||
 |
 |
 |
|
 |
 |
 |
|
These images are an example of practical non-invasive imaging technologies that are currently used worldwide. The Doppler blood flow has been used for 30 years in Europe and Japan. Elastography (also non-invasive modality to show how hard or malignant a tumor is) has been around for 15 years with great success in many countries. A benign looking elastogram scan avoids biopsies in the thyroid, breast, prostate and lymph nodes. While elastography is relatively new in the United States, the addition of Pet/CT with digital analysis is adding further specificity because chemotherapy, filler and benign tumors can show up as positive findings on a pet CT scan- we have to make sure that what's showing up as a bright lesion is not a false positive. The addition of documenting a hot area on the isotope Pet/CT scan is important to avoid false positives. The latest digital Pet/CT scans are more accurate and quantify true positives and allow you to avoid biopsying false positives. The orchestra of multiple complimentary non-invasive imaging technologies assures a quick and accurate way of determining cancer aggression and accurately allowing you to adjust treatment as needed in a timely matter. |
|||


|
|||||||||||||||||
FAQ about Non-Invasive Sonic Technology & the Future of Cancer Biopsies Since 1973, Dr. Bard established global recognition in the medical field through his contributions in the advancement of cancer diagnostic innovations. His special use of advanced imaging technologies are widely praised as the painless alternative and a more accurate innovation as well as a much faster solution for acquiring results over surgical biopsies. For the patient, it's a world of difference and immediate peace of mind when the 3D imaging establishes the diagnosis during the examination as you literally see the pictures in front of you in real time. Q: How accurate is Advanced Sonography in identifying cancers? (open) Q: Give us an example of your 4D Scan's accuracy over conventional diagnostic methods? (open) Q: What types of cancers are most commonly captured with this technology? (open) Q: How can digital scanning be instrumental in Early Detection? (open) Q: What are the benefits of using the Doppler Ultrasound imaging for BREAST CANCER? (open) Q: Why scan the lymph nodes in the axillae? (open) Q: What are the most recent upgrades in the cancer imaging industry? (open) Q: Can this technology be useful in other health issues and disorders? (open)
|
|||||||||||||||||
 |
|||||||||||||||||

 BREAST CANCER SCREENING REGIMEN
BREAST CANCER SCREENING REGIMEN|
COMPUTERIZED 3D DOPPLER HISTOGRAM ANALYSIS
For more information or to subscribe to our EARLY CANCER DETECTION & PREVENTION PROGRAM newsletter, contact Bard Cancer Diagnostics today at: 212.355.7017 - or email us at: bardcancercenter1@gmail.com. Bard Cancer Diagnostics is located at 121 E. 60th St. Suite #6A New York, NY 10022. Visit the complete website: www.CancerScan.com
|

 As of Jan '18, Dr. Robert Bard spearheaded a partnership with a host of cancer educators, medical practitioners and non-profit foundations (allied under
As of Jan '18, Dr. Robert Bard spearheaded a partnership with a host of cancer educators, medical practitioners and non-profit foundations (allied under EARLY DETECTION SAVES LIVES!
|
 |